Digital technology and data are welcomed by NHS professionals. However, it is the financial exploitation of data which needs to be considered carefully. Is data being used to improve healthcare for patients, or to improve profitability for private providers or insurance companies?
In the Information Age, the value of NHS data may well be greater than the value of NHS land. The vulnerability of the public purse to corporate exploitation of our data will be far in excess what we’ve experienced through the Public Finance Initiative.
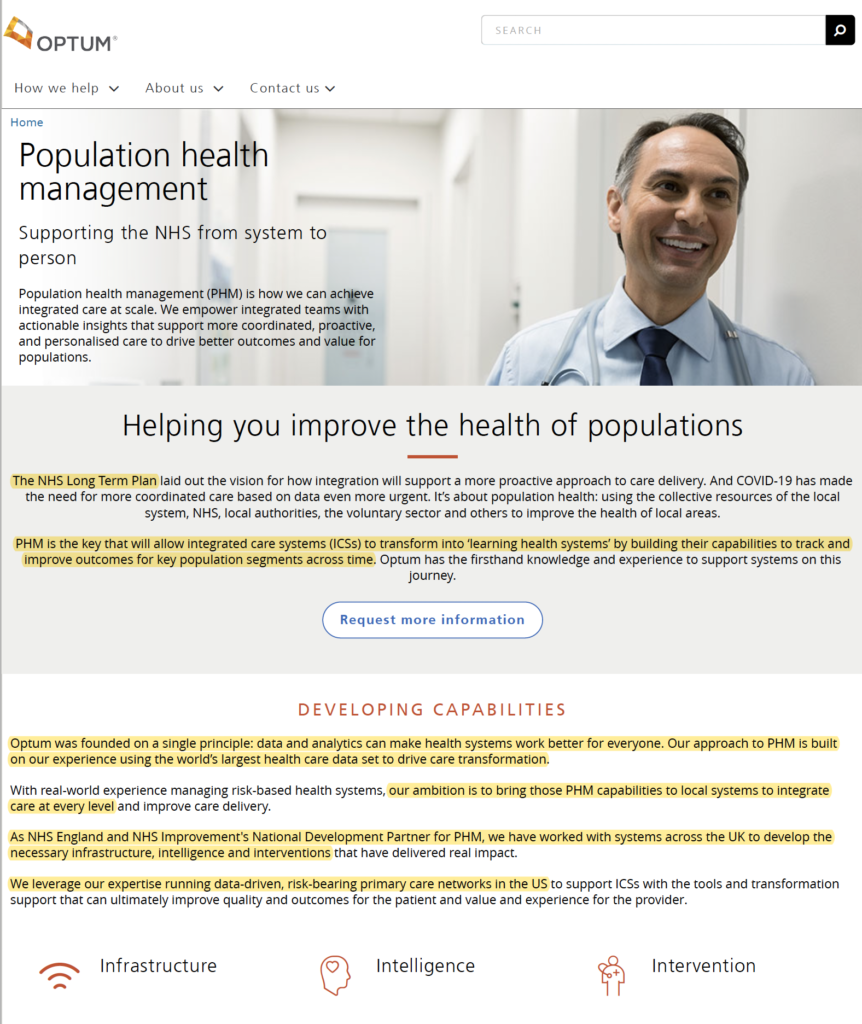
It’s important to realise that currently NHS England’s National Development Partner for using data and analytics to promote Integrated Care Systems is Optum UK – a front company for United Healthcare, the US’s largest private healthcare insurance company and the former employer of Simon Stevens.
If Optum or other private corporations control our healthcare data (or even if they control the interpretation of it), then large regional integrated care systems managing the health and social care of millions of people will be unable to function without those private corporations.
Given serious questions about contracts given to Google DeepMind, Amazon and Babylon Health, the mismanagement of data during the Test & Trace scheme, and recent public dismay about proposals to share primary care data without the explicit consent of patients, it’s important that we ensure our data is exploited for our benefit.





This is a consequence of a government that at its heart is for and supported by big business and not for all the people. It is a capitalist party that evidently benefited those with most to gain from their system of essential social economic survival of the fittest. This is not for the masses despite gaslighting the so called northern England red wall electorate with levelling up infrastructure investment white elephants that ultimately like HS2 will not materialise but makes good positive political capital sound bites and appears invested.
What is happening is not so much under the radar as freedom day is pushed to provide saturation cover while the new healthcare minister being not only the ex chancellor but also from a business investment banking background is brought in to effectively borrowing their terminology “streamline” the NHS and social care. Basically this simply means leveraging the current NHS state system to sell off or increasingly partner with big global healthcare businesses (eg USA pharmaceutical giants to sweeten a potential UK USA “free” trade deal) in a continuation towards a hybrid public private national healthcare business model.
It’s nothing new and not unexpected. Basically the person on the street in England being of relatively modest analytical ability. I say this in a factual and not arrogant manner as let’s be frank – our under funded state schools and some colleges or newer universities are not exactly world beating when benchmarked against the likes of Singapore or Finland etc.
The government will use the pandemic as cover to essentially take the opportunity to make material changes which will be disadvantageous to the general public accustomed to the current all you can eat free at point of use (and abuse) tax payer funded business model. Essentially we can’t afford to run and fund this business model for national healthcare because the demand from the pandemic as well as regular demand will massively out strip the supply capacity. In addition we are about to come to turns with economic realities. Our current national debt at apparently close to GDP is unsustainable despite much of this being calculated as a multigenerational long term war debt that will not require paying off for decades so essentially not this government’s problem as they will be long gone to clear up any mess created now.
So why are people astonished with a strategic plan to semi privatise healthcare when now will be the busiest ever demand customer base by stealth dressed up as national healthcare optimisation because of the opportunities perfectly presented by a global pandemic. This government can claim to be a world beating vaccination government while at the same time rape and fill their boots with off the scale once in a lifetime opportunity to personally profit and get their mates on board an unlimited gravy train eating our monies we technically don’t have through national borrowing.
Oh and finally the current corrupt gaslighting unfit for purpose government (with a large parliamentary majority) will fudge not just to remove the statutory duty to provide hospital medical services but simply say this is a necessity of pandemic and post pandemic healthcare as this new framework would be more efficient with market competitive elements and new fit for purpose healthcare system in keeping with USA and most other advance nations that do not have “free all you can eat birth to end of life cycle” healthcare.
So predictable folks as nothing to shock here but English populace taking Covid risks because accustomed to free medical treatment if needed with no understanding nor appreciation of the true market price and cost of the medical care they take for granted as freebies. This is reflected in our per capita Covid statistics as people in most overseas nations take personal and mutual community civic duty of care Covid risk mitigation measures seriously and less blasé because otherwise they will like in developing counties, finally realise oxygen is not only in short supply but expensive in a global respiratory pandemic!
I guess people will now be annoyed that you were saving the NHS as much to save lives as a system that can be repurposed and repackaged for profit too at your health disadvantage.
Dust storm created by other newsworthy items like Racism and the Pandemic have sadly given cover for this latest Bill to be rushed through. We need the mainstream media to step up and publicise the pitfalls. BBC DO YOUR DUTY.
This is an excellent summary of a unnecessary complicated NHS white paper sadly highlighting US Health Insurance Companies profiteering by being offerd the coffin nails of our NHS. In other words give away or sell the nails the wood and the coffin become useless as my mother would have said.
Last chance to Save our NHS when it’s gone it’s gone people. Never Trust a Tory with planning your health care, unless you’ve got a huge pot of money to pay for it!!
This plan to reorganise the NHS is full of ambiguity.,this government s usual slight of hand manoeuvre s .
Try to pull the wool over our eyes as they think the general public are stupid and not notice that they are trying to privatise our service by the back door as the Tory aim has always been to pull down this well respected and loved institution from day one.
This reorganisation must be done at a proper rate of expediency with all decisions being open and above board ,giving the tax payers a fully transparent overview